Jul 2023
Lipoma
Reviewer(s): Dharam Ramnani, MD | Last Update: 7/23/2023
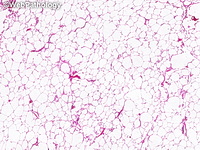
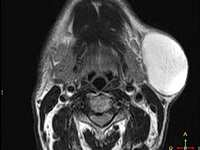
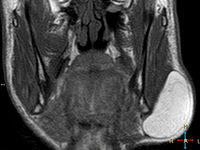
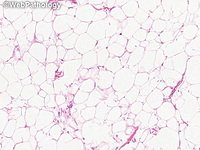
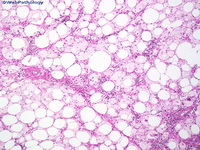
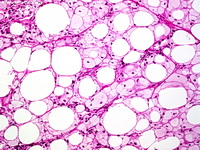
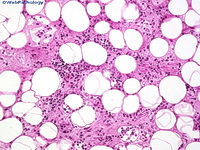
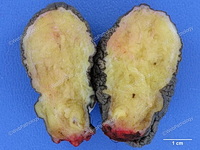
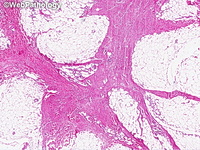
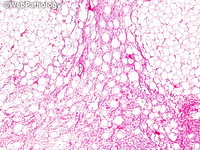
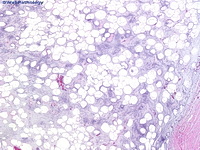
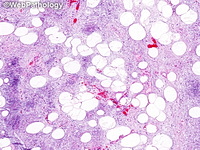
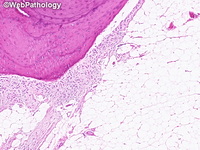
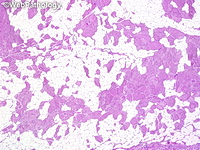
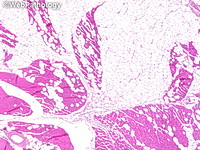
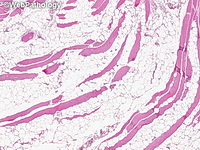
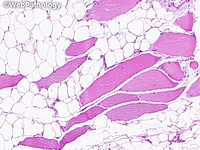
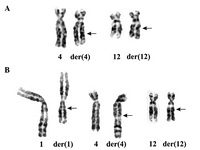
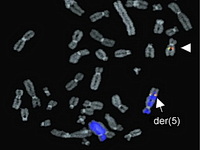
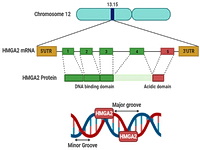
Solitary lipoma is the most common soft tissue tumor. It is slow-growing and rarely poses significant clinical problems. About 5% of patients have multiple lipomas, many of which have hereditary predisposition. Most lesions arise in the subcutaneous tissues of upper back, neck, shoulder, abdomen, buttocks, upper thigh and upper arm. Infrequently, they occur in the deep soft tissues or specific anatomic sites. Both CT and MRI are excellent imaging modalities for the diagnosis of lipomas. On MRI, they show high signal intensity on T1-weighted images. Grossly, superficial lipomas are small, well-circumscribed, round to oval masses with a thin capsule. The deeper lipomas are larger and more irregular in shape. The cut surface is homogenous, greasy and pale yellow to orange. Microscopically, they show lobules of variably-sized mature fat cells and a delicate vascular network. There is no nuclear hyperchromasia. Lipoma variants contain mesenchymal elements such as fibrous tissue (fibrolipoma) or myxoid stroma (myxolipoma). Most lipomas show structural rearrangements of 12q13-15, usually in the form of translocation t(3;12)(q27-28;q13-15), targeting the HMGA2 gene. Less commonly, the translocations involve 12q13-15 and other chromosomes (1p, 2p, 2q, 5q, 11q, and 12p).