
Silicone Lymphadenopathy : Microscopic



Comments:
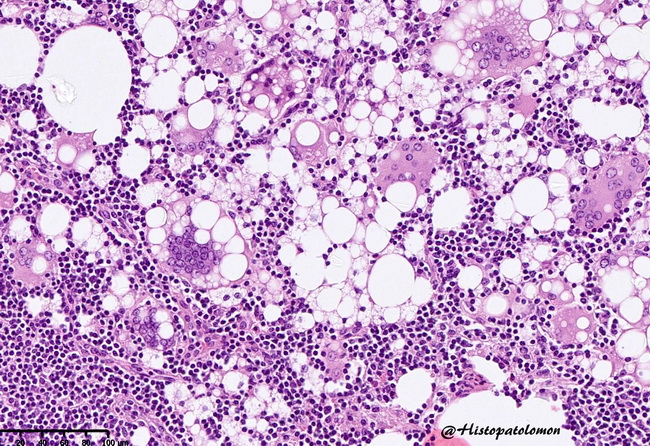
Microscopic Features of Silicone Lymphadenopathy: The extent of lymph node involvement is variable and ranges from patchy (most common) to diffuse (uncommon). Follicular hyperplasia is usually present. The reaction to silicone depends upon the polymer size. Liquid silicone (short chain polymer) causes minimal cellular reaction. Larger silicone particles, such as silicone rubber composed of cross-linked long chains, is associated with foreign body giant cell response. There are round vacuoles of varying sizes within nodal parenchyma, creating a lace-like appearance at low magnification. Silicone may be washed away during specimen processing and the vacuoles appear empty or there may be refractile, non-birefringent, and colorless particles within the vacuoles (see the large vacuole on the upper left). Histiocytes phagocytose silicone resulting in bubbly or frothy cytoplasm. Aggregates of such histiocytes are commonly seen in sinusoidal region of the affected lymph nodes. Non-necrotizing granulomas with epithelioid and foreign body giant cells are generally caused by material other than silicone, such as polyurethane, which is commonly present in the implants. Silicone lymphadenopathy usually does not show fibrosis, necrosis, cytologic atypia or increased mitotic activity. Asteroid bodies may be seen in the cytoplasm of epithelioid or giant cells in silicone lymphadenopathy. They appear as eosinophilic, stellate or spider-like inclusions with radiating filamentous arms that contain complex lipoproteins, calcium, phosphorus, silicon, and aluminum. Besides silicone lymphadenopathy, asteroid bodies are also seen in sarcoidosis and other lymphadenopathies. Image courtesy of: Pascual Meseguer (@histopatolomon); used with permission.