Miscellaneous Bladder Tumors
High Quality Pathology Images of Genitourinary: Urinary Bladder of Miscellaneous Bladder Tumors
Home
Sections
Neuropath
Glial Tumors
Non-Glial Tumors
Non-Neoplastic
Breast
Benign Prolif. Lesions
Breast Carcinomas
Rare Breast Tumors
Inflammatory/Reactive
Head & Neck
Oral Cavity, Oropharynx & Neck
Maxillofacial
Salivary Glands
Nose & Sinuses
Larynx
Ear
Eye
Mediastinum
Mediastinum
Peritoneum
Peritoneum, Omentum & Mesentery
Genitourinary
Prostate
Urinary Bladder
Kidney
Testis
External Genitalia
Adrenal
Cancer Genomics
Soft Tissue Tumors
Hematopathology
Mature B-cell Neoplasms - Part I
Mature B-cell Neoplasms - Part II
Mature T-cell & NK-cell Neoplasms
Myeloid, Histiocytic & Dendritic Cell Neoplasms
Lymph Node (Non-Hematopoietic)
Spleen
Gynecologic
Vulva/Vagina
Cervix
Uterus
Ovary
Placenta & Trophoblastic Lesions
Orthopedic
Bone Tumors - I
Bone Tumors - II
Tumor-like Lesions of Bone
Misc. Bone Lesions
Lesions of Joints
DermPath
Proliferations & Neoplasms
Non-Neoplastic DermPath - I
Non-Neoplastic DermPath - II
Endocrine
Thyroid
Parathyroid
Pancreas
Adrenal
Pituitary
Gastrointestinal
Esophagus
Stomach
Small Bowel
Appendix
Large Bowel
Anus
Liver
Gallbladder
Pancreas
Soft Tissue
Fibroblastic
Fibrohistiocytic
Lipomatous
Myogenic
Vascular & Lymphatic
Peripheral Nerve
Uncertain Histogenesis
Misc. Soft Tissue Lesions
Pulmonary
Lung - Non-Neoplastic
Epithelial Lung Tumors
Mesenchymal Tumors of Lung
Pleura
Miscellaneous Lung Tumors
Cardiovascular
Heart
Blood Vessels
Infectious Disease
Specific Clinical Syndromes
Gram-Positive Bacteria
Gram-Negative Bacteria - I
Gram-Negative Bacteria - II
Acid-Fast Bacilli
Yeast & Yeast-like Fungi
Filamentous Fungi (Molds)
Viruses
Parasites
Pediatric
Pediatric Pathology - I
Pediatric Pathology - II
Cytopathology
Cytopathology 1
Cytopathology 2
Genetic Disorders
About
Feedback
Contact
Striving to be the most comprehensive online resource for high-quality pathology images
13,153
Images
Miscellaneous Bladder Tumors
Reviewer(s): Dharam M. Ramnani, M.D.
Home
Genitourinary
Urinary Bladder
Miscellaneous Bladder Tumors
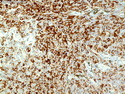
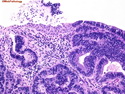
Lymphoma in Urinary Tract
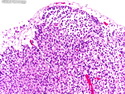
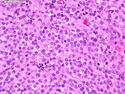
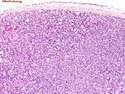
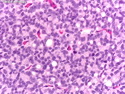
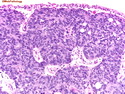
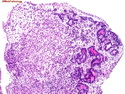
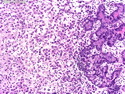
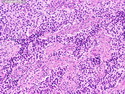
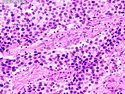
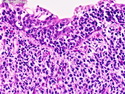
Primary Lymphoma of Bladder
Primary Lymphoma of Bladder
Primary Lymphoma of Bladder
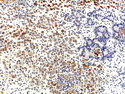
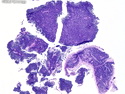
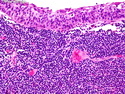
Secondary Lymphoma involving Ureter
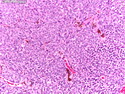
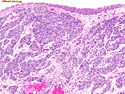
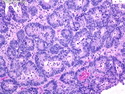
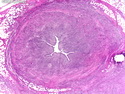
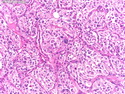
Paraganglioma of Bladder
Paraganglioma of Bladder
Paraganglioma of Bladder
Paraganglioma of Bladder
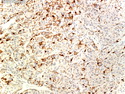
Paraganglioma of Bladder : S100
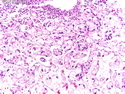
Metastases : Melanoma
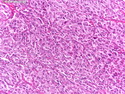
Metastatic Melanoma in Bladder
Metastatic Melanoma in Bladder
Metastatic Melanoma in Bladder
Metastatic Melanoma in Bladder
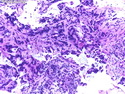
Metastases : Prostate Cancer
Metastatic Prostate Cancer in Bladder
Metastatic Prostate Cancer in Bladder
Metastatic Prostate Cancer in Bladder
Metastatic Prostate Cancer in Bladder
Metastatic Prostate Cancer in Bladder : PSA Immunostain
Metastatic Prostate Cancer in Bladder
Metastatic Prostate Cancer in Bladder
Metastatic Prostate Cancer in Bladder
Metastases : Colorectal Adenocarcinoma
Metastatic Colorectal AdenoCA in Bladder
Metastatic Colorectal AdenoCA in Bladder
Metastatic Colorectal AdenoCA in Bladder
Metastatic Colorectal AdenoCA in Bladder
Metastases : Seminoma
Metastatic Seminoma in Bladder
Metastatic Seminoma in Bladder

.jpg)