Ductal Carcinoma-in-situ
High Quality Pathology Images of Breast: Breast Carcinomas of Ductal Carcinoma-in-situ
Home
Sections
Neuropath
Glial Tumors
Non-Glial Tumors
Non-Neoplastic
Breast
Benign Prolif. Lesions
Breast Carcinomas
Rare Breast Tumors
Inflammatory/Reactive
Head & Neck
Oral Cavity, Oropharynx & Neck
Maxillofacial
Salivary Glands
Nose & Sinuses
Larynx
Ear
Eye
Mediastinum
Mediastinum
Peritoneum
Peritoneum, Omentum & Mesentery
Genitourinary
Prostate
Urinary Bladder
Kidney
Testis
External Genitalia
Adrenal
Cancer Genomics
Soft Tissue Tumors
Hematopathology
Mature B-cell Neoplasms - Part I
Mature B-cell Neoplasms - Part II
Mature T-cell & NK-cell Neoplasms
Myeloid, Histiocytic & Dendritic Cell Neoplasms
Lymph Node (Non-Hematopoietic)
Spleen
Gynecologic
Vulva/Vagina
Cervix
Uterus
Ovary
Placenta & Trophoblastic Lesions
Orthopedic
Bone Tumors - I
Bone Tumors - II
Tumor-like Lesions of Bone
Misc. Bone Lesions
Lesions of Joints
DermPath
Proliferations & Neoplasms
Non-Neoplastic DermPath - I
Non-Neoplastic DermPath - II
Endocrine
Thyroid
Parathyroid
Pancreas
Adrenal
Pituitary
Gastrointestinal
Esophagus
Stomach
Small Bowel
Appendix
Large Bowel
Anus
Liver
Gallbladder
Pancreas
Soft Tissue
Fibroblastic
Fibrohistiocytic
Lipomatous
Myogenic
Vascular & Lymphatic
Peripheral Nerve
Uncertain Histogenesis
Misc. Soft Tissue Lesions
Pulmonary
Lung - Non-Neoplastic
Epithelial Lung Tumors
Mesenchymal Tumors of Lung
Pleura
Miscellaneous Lung Tumors
Cardiovascular
Heart
Blood Vessels
Infectious Disease
Specific Clinical Syndromes
Gram-Positive Bacteria
Gram-Negative Bacteria - I
Gram-Negative Bacteria - II
Acid-Fast Bacilli
Yeast & Yeast-like Fungi
Filamentous Fungi (Molds)
Viruses
Parasites
Pediatric
Pediatric Pathology - I
Pediatric Pathology - II
Cytopathology
Cytopathology 1
Cytopathology 2
Genetic Disorders
About
Feedback
Contact
Striving to be the most comprehensive online resource for high-quality pathology images
13,153
Images
Dec 2015
Ductal Carcinoma-in-situ
Home
Breast
Breast Carcinomas
Ductal Carcinoma-in-situ
DCIS
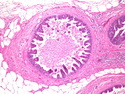
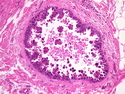
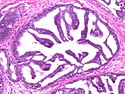
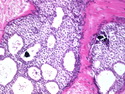
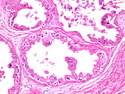
Ductal Carcinoma-in-situ : Micropapillary
Ductal Carcinoma-in-situ : Micropapillary
Ductal Carcinoma-in-situ : Micropapillary
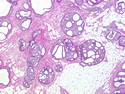
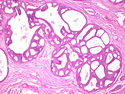
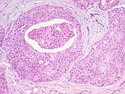
Ductal Carcinoma-in-situ : Cribriform
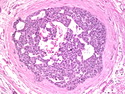
Ductal Carcinoma-in-situ : Cribriform with Microcalcifications
Ductal Carcinoma-in-situ : Cribriform
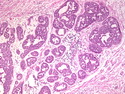
Ductal Carcinoma-in-situ
Ductal Carcinoma-in-situ
Ductal Carcinoma-in-situ : Apocrine
Ductal Carcinoma-in-situ : Comedonecrosis